 |
Case Report
Large uterine leiomyoma presenting as pseudo-Meigs’ syndrome with an elevated CA 125: Case report and literature review
1 Student, School of Medicine, The University of Texas Medical Branch, Galveston, Texas, United States
Address correspondence to:
Jake Alan Gibbons
500 Seawall Blvd Unit 1109, Galveston, Texas 77550,
United States
Message to Corresponding Author
Article ID: 100046Z08JG2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gibbons JA. Large uterine leiomyoma presenting as pseudo-Meigs’ syndrome with an elevated CA 125: Case report and literature review. J Case Rep Images Obstet Gynecol 2019;5:100046Z08JG2019.ABSTRACT
Introduction: Uterine leiomyomas presenting as pseudo-Meigs’ syndrome with an elevated CA 125 are rare and pose a diagnostic challenge for physicians.
Case Report: A 35-year-old G0P0 presented to the emergency department with a chief complaint of abdominal swelling and weight gain beginning one month ago. Laboratory work was significant for an elevated CA 125. She was found to have a large mass originating from her uterus. Following resection of the mass, her symptoms resolved. Pathology of the mass came back as a uterine leiomyoma.
Conclusion: Generally, findings of ascites, a pelvic mass, and an elevated CA 125 in a female suggests a diagnosis of ovarian cancer. However, as demonstrated by our case and others, benign causes such as Meigs’ syndrome and pseudo-Meigs’ syndrome should also be considered. Surgery is the mainstay of treatment in pseudo-Meigs’ syndrome. Resolution of the ascites and hydrothorax occurs spontaneously following resection of the tumor.
Keywords: Ascites, CA 125, Gynecology, Leiomyoma, Pseudo-Meigs’ syndrome
Introduction
Meigs’ syndrome is the triad of a benign ovarian fibroma or thecoma combined with ascites and hydrothorax [1]. A clinically similar yet distinct pathological entity is pseudo-Meigs’ syndrome. Like Meigs’ syndrome, pseudo-Meigs’ syndrome presents with ascites and hydrothorax. However, unlike Meigs’ syndrome, pseudo-Meigs’ syndrome is associated with non-thecoma, non-fibroma ovarian tumors or uterine leiomyomas [1]. Ovarian tumors reported in pseudo- Meigs’ syndrome include: strumaovarii tumors, germ cell tumors, ovarian metastases from gastric or colon cancer, and serous or mucinous cystadenomas [2]. The uterine leiomyoma, however, is the most commonly reported tumor in cases of pseudo-Meigs’ syndrome [3]. Leiomyomas have an incidence of 20-50% in females over the age of 30, but only rarely do they present with ascites and hydrothorax [1]. On its own, pseudo-Meigs’ syndrome is a rare diagnosis. A concomitant elevation in cancer antigen 125 (CA 125) in a patient presenting with pseudo- Meigs’ syndrome is an even more uncommon finding [4],[5],[6],[7]. We report a case of pseudo-Meigs’ syndrome in a 35-year-old female who was also found to have a markedly elevated CA 125. Additionally, a literature review was performed and past cases of pseudo-Meigs’ syndrome were identified. Data from those cases is presented in the discussion section of this paper following the case report.
Case Report
A 35-year-old G0P0 who presented to the emergency department with a chief complaint of abdominal swelling and weight gain beginning one month ago. She reported increasing abdominal pain, abdominal swelling, nausea, and vomiting. She denied chest pain, shortness of breath, heat or cold intolerance, palpitations, and any motor or sensory deficits. She had no history of cancer. Her past surgical history was significant for an exploratory laparotomy sixteen years ago due to an abdominal stab wound.
On physical examination, her abdomen was distended and mildly tender to palpation in all four quadrants. A fluid wave was present. A large mass was palpated in the left lower quadrant. No other abnormalities were observed on physical examination. Her blood work was significant for a leukocyte count of 12.8 103/µL and a markedly elevated CA 125 level of 272.9 U/ml. Given the elevated CA 125, combined with the ascites and mass on physical examination, a presumptive diagnosis of ovarian carcinoma was made.
A CT scan was ordered, which demonstrated a large intra abdominal mass measuring 28.8 cm and significant ascites. The mass contained both cystic and solid components, as well as internal vascularity. Omental carcinomatosis was also present.
The patient was taken to the operating room for a planned exploratory laparotomy, lysis of adhesions, omentectomy, excision of intra abdominal mass, hysterectomy, and bilateral salpingo-oophorectomy. An incision was made from the diploid process to the symphysis pubis. The wound was deepened using electrocautery. Upon entry into the abdomen, two ventral hernias were identified. The hernia sacs were divided and sent to pathology. Two liters of intra abdominal fluid was aspirated. Peritoneal washings were sent to pathology.
The mass was identified. It was closely adherent to the anterior abdominal wall, and also involved the omentum, sigmoid colon, and two large areas of small bowel. It was dissected from the anterior abdominal wall and the two segments of small bowel. Both of the segments of small bowel were resected. Two side-to-side functional end-toend anastomoses were performed to close the common enterotomy.
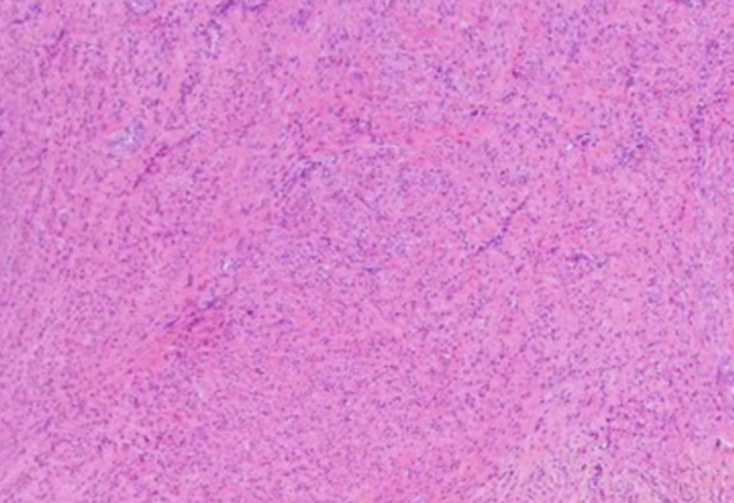
A portion of the sigmoid mesentery involving the mass was removed. The tumor, which appeared to originate from the uterine fundus, was completely resected and sent to pathology. A total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed. The abdomen was examined for additional sites of metastasis, but none were identified. The abdomen was closed using #1 looped Polydiaxanone sutures. The wound was irrigated with saline and subsequently closed with a skin stapler. The patient tolerated the procedure well and was extubated without complications. Pathology demonstrated that the mass was an aggressive-behaving uterine leiomyoma (Figure 1). Additionally, ascitic cytology was negative for malignant cells.
Discussion
Findings of ascites, a pelvic mass, and an elevated CA 125 in a female carry a grim prognosis, most likely that of an ovarian carcinoma [8],[9]. However, as demonstrated by this case and others, benign etiologies must also be considered on the differential diagnosis [9]. Cases of Meigs’ syndrome and pseudo-Meigs’ syndrome with elevations in CA 125 have been reported, which should prompt physicians to consider these diagnoses as well [9],[10],[11]. Furthermore, an elevated CA 125 is not 100% specific for ovarian carcinoma [12]. Pelvic inflammatory disease, pregnancy, endometriosis, benign ovarian tumors, and uterine leiomyomas can cause CA 125 to become elevated [13]. In cases of Meigs’ syndrome, it has been conjectured that mesothelial expression of CA 125, as opposed to expression by the fibroma, is the cause of the elevation [10],[11]. In pseudo-Meigs’ syndrome, peritoneal inflammation has been implicated as the cause of the elevation in CA 125 [9].
In both Meigs’ syndrome and pseudo-Meigs’ syndrome, spontaneous resolution of the pleural effusion and ascites occurs following resection of the underlying tumor [14]. The cause of the ascites and hydrothorax in both Meigs’ syndrome and pseudo-Meigs’ syndrome is not entirely known, but likely multifactorial. It has been reported that, intraoperatively, cutting a uterine leiomyoma caused fluid leakage from myometrial cysts within the tumor [9]. Thus, it is possible that the fluid production is the result of cystic degeneration of the tumor [15]. In addition to fluid from the tumor itself, peritoneal fluid production is also a likely factor in the production of the ascites. Mechanical irritation of the peritoneum from the tumor in addition to pressure from pre-existing ascites causes peritoneal inflammation, which results in further fluid production [16]. The development of pleural effusion in these syndromes is thought to be a result of transdiaphragmatic transport of the ascitic fluid into the thorax through intercellular gaps [9].
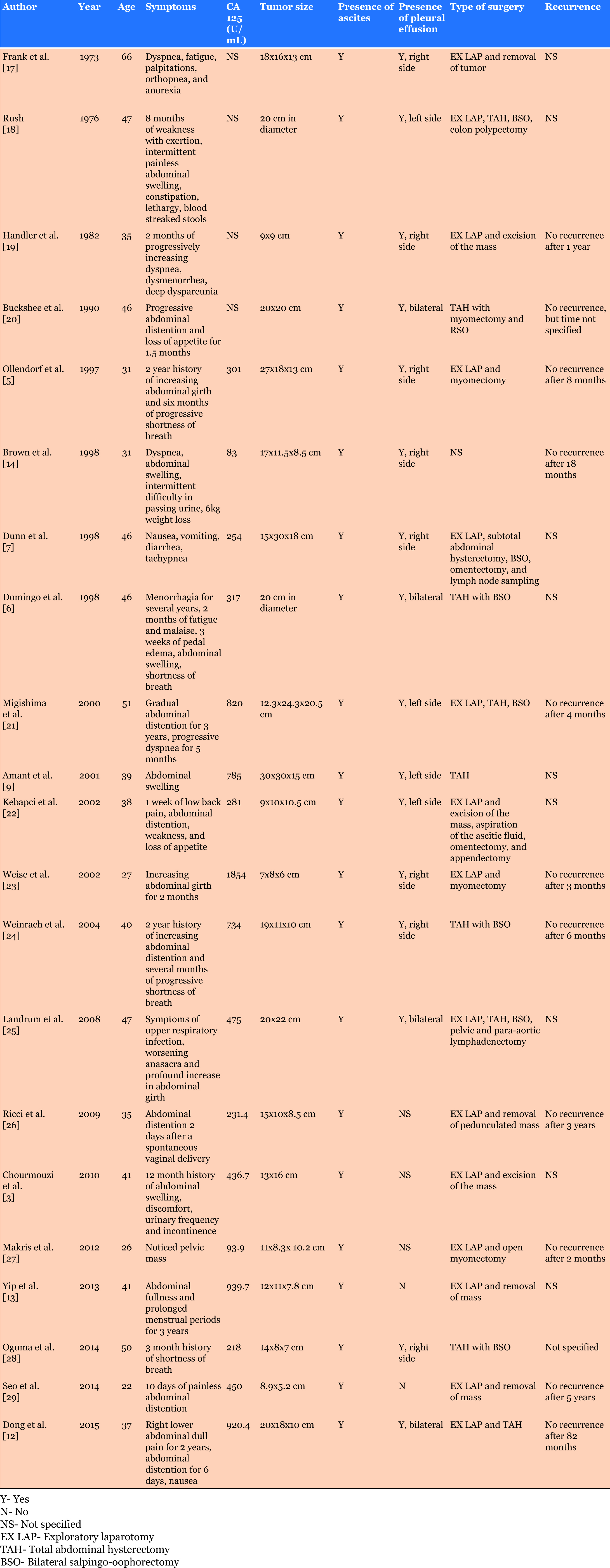
A comprehensive review of the English literature using PubMed and Medline was performed, which resulted in 21 cases describing uterine leiomyomas presenting as pseudo-Meigs’ syndrome with an elevated CA 125 (Table 1). Review of the literature indicates that the mean age of presentation was 40 years (22–66 years). The majority of patients, 15 of 21 cases, presented with abdominal distention. Additionally, in 8 of 21 cases, patients reported dyspnea. Other symptoms less commonly reported include: nausea, vomiting, dysuria, and urinary frequency. The average CA 125 level of the 21 cases was 541 U/mL (83 U/mL-1854 U/mL). Ascites was present in all 21 cases, and hydrothorax was reported in 16 of the 21 cases. All patients were treated surgically, with no reported cases of tumor recurrence.
Conclusion
Uterine leiomyomas presenting as pseudo-Meigs’ syndrome with an elevated CA 125 are exceedingly rare. In a patient with a clinical presentation consistent ovarian cancer with the added finding of an elevated CA 125, benign etiologies such as Meigs’ syndrome and pseudo-Meigs’ syndrome should also be considered in the differential diagnosis. Surgery is the mainstay of treatment in pseudo-Meigs’ syndrome. Resolution of the ascites and hydrothorax occurs spontaneously following resection of the tumor. No cases of recurrence have been reported in the literature.
REFERENCES
1.
Meigs JV. Fibroma of the ovary with ascites and hydrothorax; Meigs' syndrome. Am J Obstet Gynecol 1954;67(5):962–85.
[Pubmed]

2.
Zannoni GF, Gallotta V, Legge F, Tarquini E, Scambia G, Ferrandina G. Pseudo-Meigs' syndrome associated with malignant struma ovarii: A case report. Gynecol Oncol 2004;94(1):226–8. [CrossRef]
[Pubmed]
3.
Chourmouzi D, Papadopoulou E, Drevelegas A. Magnetic resonance imaging findings in pseudo-Meigs' syndrome associated with a large uterine leiomyoma: A case report. J Med Case Rep 2010;4:120. [CrossRef]
[Pubmed]
4.
Lee MJ, Kazer RR. Massive ascites after leuprolide acetate administration for the treatment of leiomyomata uteri. Fertil Steril 1992;58(2):416–8.
[Pubmed]
5.
Ollendorff AT, Keh P, Hoff F, Lurain JR, Fishman DA. Leiomyoma causing massive ascites, right pleural effusion and respiratory distress: A case report. J Reprod Med 1997;42(9):609–12.
[Pubmed]
6.
Domingo P, Montiel JA, Monill JM, Prat J. Pseudo-Meigs syndrome with elevated CA 125 levels. Arch Intern Med 1998;158(12):1378–9.
[Pubmed]
7.
Dunn JS Jr, Anderson CD, Method MW, Brost BC. Hydropic degenerating leiomyoma presenting as pseudo-Meigs syndrome with elevated CA 125. Obstet Gynecol 1998;92(4 Pt 2):648–49.
[Pubmed]
8.
Gal D, Buchsbaum HJ, Voet R, Forney JP. Massive ascites with uterine leiomyomas and ovarian vein thrombosis. Am J Obstet Gynecol 1982;144(6):729– 31. [CrossRef]
[Pubmed]
9.
Amant F, Gabriel C, Timmerman D, Vergote I. Pseudo-Meigs' syndrome caused by a hydropic degenerating uterine leiomyoma with elevated CA 125. Gynecol Oncol 2001;83(1):153–7. [CrossRef]
[Pubmed]
10.
Lin JY, Angel C, Sickel JZ. Meigs syndrome with elevated serum CA 125. Obstet Gynecol 1992;80(3 Pt 2):563–6.
[Pubmed]
11.
Timmerman D, Moerman P, Vergote I. Meigs' syndrome with elevated serum CA 125 levels: Two case reports and review of the literature. Gynecol Oncol 1995;59(3):405–8. [CrossRef]
[Pubmed]
12.
Dong R, Jin C, Zhang Q, Yang X, Kong B. Cellular leiomyoma with necrosis and mucinous degeneration presenting as pseudo-Meigs' syndrome with elevated CA125. Oncol Rep 2015;33(6):3033–7. [CrossRef]
[Pubmed]
13.
Yip HK, Huang LW, Lin YH, Hwang JL. Massive ascites caused by a large pedunculated subserosal uterine leiomyoma that has feeding arteries from peripheral tissues and exhibits elevated CA125: A case report of atypical pseudo-Meigs' syndrome. J Obstet Gynaecol 2014;34(1):107. [CrossRef]
[Pubmed]
14.
Brown RS, Marley JL, Cassoni AM. Pseudo-Meigs' syndrome due to broad ligament leiomyoma: A mimic of metastatic ovarian carcinoma. J Clin Oncol (R Coll Radiol) 1998;10(3):198–201. [CrossRef]
[Pubmed]
15.
Clement PB. Pure mesenchymal tumors. In: Clement PB, Young RH. Tumors and Tumorlike Lesions of the Uterine Corpus and Cervix. New York: Churchill Livingstone; 1993. p. 285–328.
16.
Jimerson SD. Pseudo-Meigs's syndrome. An unusual case with analysis of the effusions. Obstet Gynecol 1973;42(4):535–7.
[Pubmed]
17.
Frank N, Frank MJ. Uterine tumour mimicking Meigs' syndrome (intractable heart failure). J Med Soc N J 1978;70(1):17–8.
[Pubmed]
18.
Rush BM. Leiomyoma of the uterus, ascites and hydrothorax (pseudo-Meig's syndrome). J La State Med Soc 1976;128(1):7–8.
[Pubmed]
19.
Handler CE, Fray RE, Snashall PD. Atypical Meigs' syndrome. Thorax 1982;37(5):396–7.
[Pubmed]
20.
Buckshee K, Dhond AJ, Mittal S, Bose S. Pseudo-Meigs' syndrome secondary to broad ligament leiomyoma: A case report. Asia Oceania J Obstet Gynaecol 1990;16(3):201–5.
[Pubmed]
21.
Migishima F, Jobo T, Hata H, et al. Uterine leiomyoma causing massive ascites and left pleural effusion with elevated CA 125: A case report. J Obstet Gynecol Res 2000;26(4):283–7.
[Pubmed]
22.
Kebapci M, Aslan O, Kaya T, Yalcin OT, Ozalp S. Pedunculated uterine leiomyoma associated with pseudo-Meigs' syndrome and elevated CA-125 level: CT features. Eur Radiol 2002;12 Suppl 3:S127–9.
[Pubmed]
23.
Weise M, Westphalen S, Fayyazi A, Emons G, Krauss T. Pseudo-Meigs syndrome. Uterine leiomyoma with bladder attachment associated with ascites and hydrothorax – a rare case of a rare syndrome. Onkologie 2002;25(5):443–6. [CrossRef]
[Pubmed]
24.
Weinrach DM, Wang KL, Keh P, Sambasiva Rao M. Pathologic quiz case: A 40-year-old woman with a large pelvic mass, ascites, massive right hydrothorax and elevated CA125. Arch Pathol Lab Med 2004;128(8):933–4.
[Pubmed]
25.
Landrum LM, Rutledge TL, Osunkoya AO, Mannel R. Uterine leiomyoma with associated pseudo-Meigs syndrome mimicking ovarian carcinoma. J Okla State Med Assoc 2008;101(2):38–9.
[Pubmed]
26.
Ricci G, Inglese S, Candiotto A, et al. Ascites in puerperium: A rare case of atypical pseudo-Meigs' syndrome complicating the puerperium. Arch Gynecol Obstet 2009;280(6):1033–7. [CrossRef]
[Pubmed]
27.
Makris A, Talmor A, Moyle P, Majmudar T, Abdel-Rahman H. Parasitic fibroid and pseudo-Meigs' syndrome: Co-existence of two rare entities. J Obstet Gynaecol 2012;32(4):408–9. [CrossRef]
[Pubmed]
28.
Oguma T, Yamasaki N, Nakanishi K, et al. Pseudo-Meigs' syndrome associated with hydropic degenerating uterine leiomyoma: A case report. J Obstet Gynaecol Res 2014;40(4):1137–40. [CrossRef]
[Pubmed]
29.
Seo M, Sung Jy, Cho Hj, et al. Ascites associated with uterine leiomyoma in a 22-year-old woman with systemic lupus erythematosus. Lupus 2014;23(11):1207–10. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Jake Alan Gibbons - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionMeigs JV. Fibroma of the ovary with ascites and hydrothorax; Meigs’ syndrome. Am J Obstet Gynecol 1954;67(5):962–85.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Jake Alan Gibbons. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}